On this Mother’s Day I’d like to honor the mothers by talking about Uteri, or uteruses (both are correct, btw), specifically uterine anomalies. In middle school when we first learn about sex and reproductive education in a classroom setting, we are usually shown a picture of a perfectly upside-down pear-shaped uterus, complete with two ovaries, two fallopian tubes, one cervix, and one vagina. However, we are not taught (or even told about) uterine anomalies. Truth be told, I doubt my gym teacher even knew there was such a thing.
Around 5.5% of women are born with a uterine anomaly, meaning there is an issue in the size, shape, or structure of their uterus. This is caused by the Mullerian ducts, the “primordial” foundation of a woman’s reproductive tract (fallopian tubes, uterus, cervix, superior aspect of the vagina) not developing as they should.
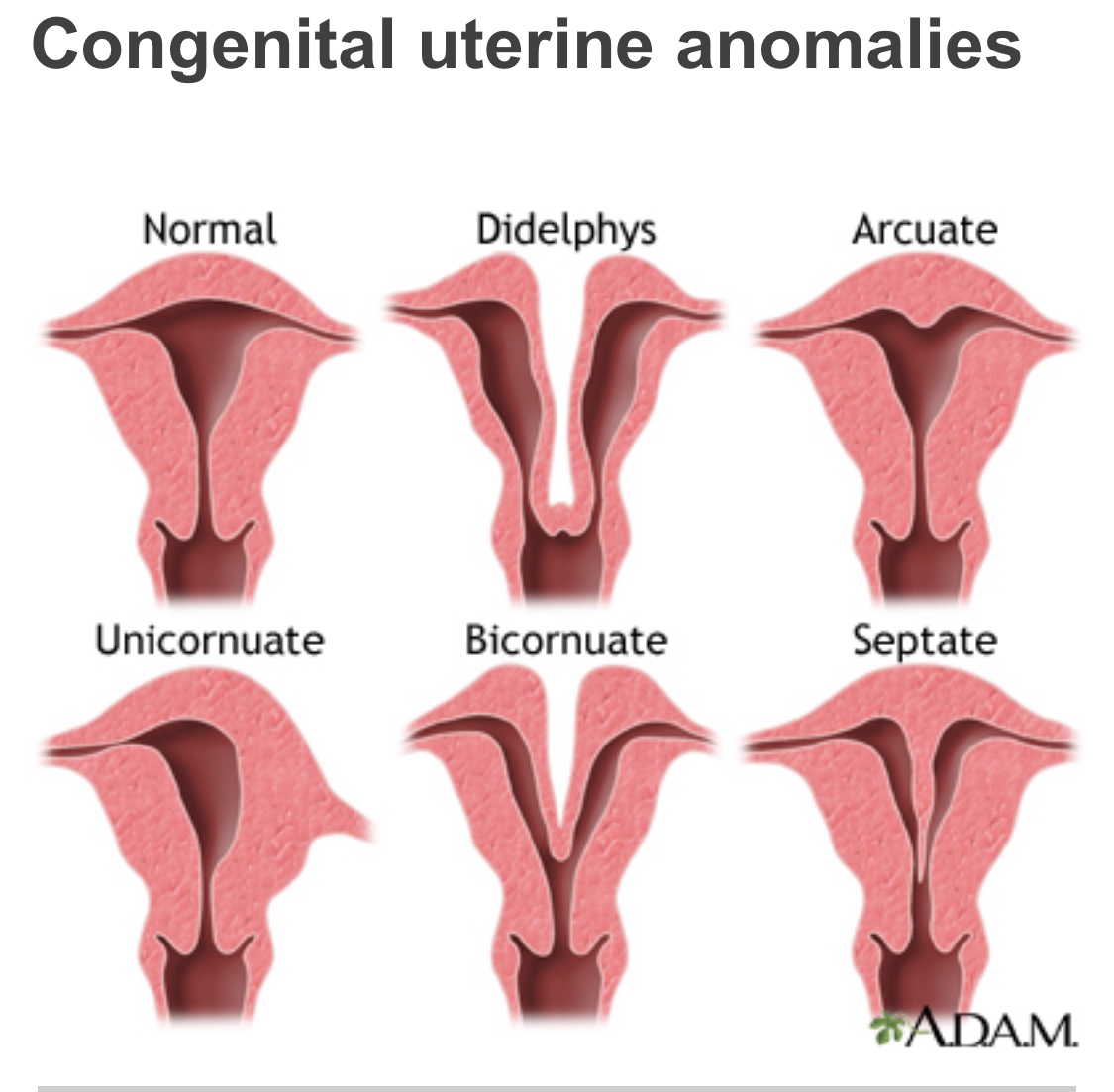
Arcuate Uterus
An Arcuate Uterus is a minor irregularity in the shape of the uterus. It’s not exactly pear-shaped; there is a small dent (a dimple if you will) in the top of the uterus. This condition has not been known to affect pregnancy or fertility. Most healthcare professionals consider it a normal uterus with a slight variation.
Septate Uterus
A Septate Uterus is divided into two parts by a membrane called the septum. It can be corrected with surgery. Some risks to pregnancy can include restricted/low birth weight, miscarriage (aka, spontaneous abortion), preterm labor (before 37 weeks of gestation), premature birth (again, a baby born before 37 weeks of gestation), breech (feet or ass first) baby, and an increased need for a c-section (probably due to breech baby). While the chance of miscarriage is higher with a septate uterus, many women have healthy pregnancies with the septum still in place. It’s the most common uterine anomaly affecting about 1% of all women.
Bicornuate Uterus
A Bicornuate Uterus is also known as a “heart-shaped” uterus. The top of the uterus dips inward in the middle of the uterus making it look like a heart (the Valentine’s Day kind, not the organ), in effect creating “two-horns.” A woman’s uterus may not expand fully, depending on the degree of separation. One degree is called a “partial bicornuate uterus” because the separation of the uterine cavity is to a lesser degree (but still heart-shaped). The second degree is called a “complete bicornuate uterus” because the separation is more distinct.
Many women are not aware they have a bicornuate uterus until they give birth and need a c-section. Other women experience several miscarriages and discover the anomaly when their doctors are looking for a cause. While many women do not have any symptoms, some do experience painful periods and repeat miscarriages.
A bicornuate uterus can affect pregnancy. It can lead to preterm labor and/or birth, low birth weight, vaginal bleeding, breech or transverse positions of the fetus (baby) leading to increased need for c-section, placenta previa (placenta partially or completely covers the cervix), and pregnancy-induced high blood pressure. A woman with a BU may require more ultrasounds to monitor the position of the baby and placenta. A bicornuate uterus is one of the more common uterine anomalies but is still a rare condition overall affecting 0.5% of women.
Didelphys Uterus
A Didelphys Uterus is a Double Uterus. A woman with this anomaly may have one cervix leading into one vagina, OR each uterine cavity may have a cervix (two cervixes). In many cases a wall of tissue runs down the length of the vagina creating two openings (i.e., TWO VAGINAS). Many women are unaware of this condition because their external genitalia appear normal. Women often find out about this anomaly when they go to the doctor to figure out why their tampon is not stopping the flow of their period. Come to find out, it’s because the tampon is only in one vagina and not the other.
Women with a double uterus often have successful pregnancies, but the condition can increase the risk of miscarriage or premature birth. It can also increase the risk of infertility and kidney problems. This anomaly affects about 0.3% of women.
Unicornuate Uterus
The final uterine anomaly on the list is, Unicornuate Uterus. I left it to last for two reasons; one it is the rarest (affecting 0.1% of women) and two I have a Unicornuate Uterus.
A unicornuate (one horn) uterus is a genetic condition in which only HALF of a woman’s uterus is formed. It is smaller and differently shaped than a ‘regular’ uterus. Instead of a pear it looks like a banana pepper. Only one fallopian tube is present (mine is on the right). Some women have a remnant horn (hemi-uterus) that may be separate from the more fully formed uterus (I don’t).
Unicornuate uterus is diagnosed either when a teenager has pain or discomfort during her periods or discovered when trying to have a baby. I had hellacious periods as a teenager, however, I wasn’t diagnosed until years later as an adult. While some women with UUs do not have a problem conceiving (problems arise due to the shape of the uterus) others need to consider intrauterine insemination or IVF.
A UU pregnancy is a high-risk pregnancy. A pregnancy that occurs in the remnant horn is much like an ectopic pregnancy. It is a MEDICAL EMERGENCY and needs to be terminated because it can lead to rupture, hemorrhage, infection, or death.
A UU pregnancy is at increased risk for miscarriage because blood flow to the uterus is only being supplied by one artery instead of two. Since the uterus is smaller and less accommodating to a growing baby it can increase the risk for second-trimester miscarriage. Other risks include, preterm labor, breech positioning, c-section, placenta previa or placental abruption, intrauterine growth restriction (small baby), preterm birth, incompetent cervix, and preterm rupture of membranes (water breaking). In fact, UUs are associated with the poorest fetal survival rate among all uterine anomalies. A few other statistics include live birth rate of 29.2%, ectopic pregnancy rate of 4%, and prematurity rate of 44%.
My Personal Experience with a UU
I was LUCKY. I experienced two first-trimester miscarriages. After miscarriage one, I had a D&C, and the doctor that performed the procedure suspected a UU. She recommended an MRI to confirm. I finally had the MRI a year later, but no one from the office called me with the results. I called the doctor’s office and was told by a receptionist if I wasn’t called then everything was normal. It was not. I was 23 and didn’t know to ask to speak to a nurse or doctor. I had another miscarriage a few years later. It wasn’t until a year or so after the second miscarriage and being unable to conceive, I had a hysterosalpingography (HSG), and there my UU was in all her banana pepper glory staring right back at me from the screen. I was officially diagnosed. Also, HSGs fucking hurt!
I was carefully monitored throughout both pregnancies. I had ultrasounds every two weeks (both of my sons were head-down every single time). I continued to work. I carried my first son to 37 weeks and 2 days. I carried my second son to 39 weeks and 3 days. I gave birth to both vaginally; son number 1 weighing in at 6lbs 14oz and number 2 weighing in at 7lbs 7oz. I was more of an exception to the UU rule, not the norm.
So… when I claim I am a Unicorn, it’s true. I have doctors’ notes to prove it.

Leave a comment